
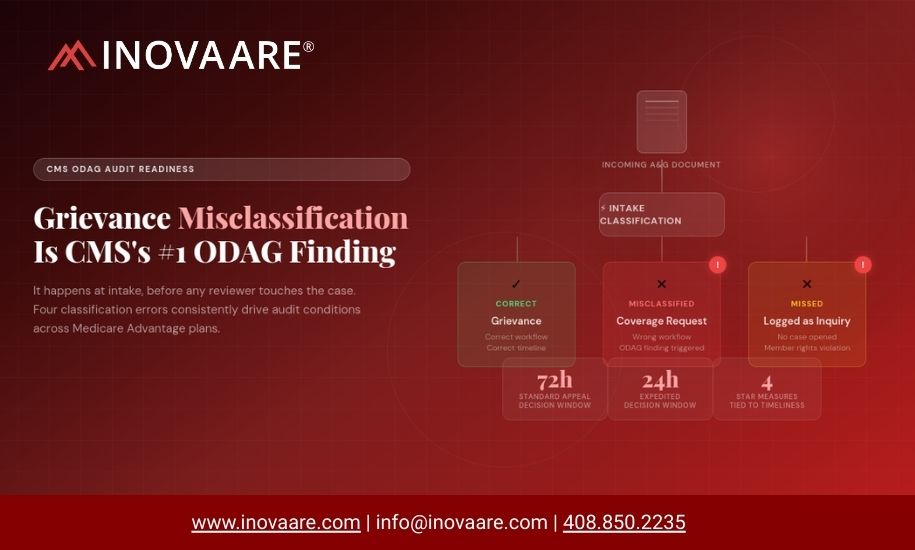
CMS auditors don’t just test timeliness — they test whether your plan correctly identified what it received in the first place. Misclassifying a grievance as a coverage request, or an appeal as an inquiry, is one of the fastest paths to an ODAG finding. And it almost always traces back to your intake process.
Every Medicare Advantage plan knows that ODAG and CDAG are two of the highest-stakes CMS program audit domains. What fewer plans fully appreciate is that the most commonly cited deficiency in both domains isn’t a decision-making failure or an effectuation gap — it’s a classification error that happens before any clinician or case manager ever looks at the case.
When a member submits a complaint about access to care, it might be a grievance. When a provider submits a request on a member’s behalf, it might be a coverage determination. When a member representative submits a document by fax, it might be an expedited appeal. Or it might be something else entirely. CMS’s ODAG audit protocol tests every one of these distinctions — and the consequences of getting them wrong compound rapidly once the wrong classification sets a case on the wrong workflow path.
“Grievances are often misclassified as coverage requests due to insufficient training of intake staff. CMS continues to see this as a vulnerability for sponsors in ODAG audits. Conduct regular monitoring and training of intake staff, review call logs, and evaluate grievance responses to ensure timely access to covered benefits and proper handling of all complaints.”
This isn’t a new finding. It has appeared consistently across ODAG and CDAG audit cycles for years. And CMS’s expansion to annual audits of all 550 MA contracts means that plans which have previously gone years between formal audits are now in scope — whether or not they’ve addressed this structural vulnerability in their intake process.
Why Classification Is the Foundational ODAG Risk
The stakes of misclassification aren’t just about the finding itself. They cascade. When a grievance is classified as a coverage request, it gets routed to the wrong workflow, measured against the wrong timeliness standards, and generates the wrong member communication. When CMS auditors pull the case universe and compare the plan’s classification against CMS’s own classification criteria, what appeared to be a timeliness issue may actually be a classification-driven miscount in the plan’s universe — creating a data integrity problem that can affect Star Ratings in addition to the program audit finding.
The reason classification errors are so persistent is structural. Most health plans receive A&G cases through multiple channels simultaneously: fax, mail, phone, email, web portal, and EDI. Each channel produces a different document type with different formatting, different completeness levels, and different contextual cues. A manual intake process — where a staff member reads an incoming document and assigns a case type — is inherently inconsistent at volume. Training helps, but training degrades as staff turns over, volumes spike, and the regulatory definitions for grievances, coverage requests, and appeals continue to evolve with each CMS guidance update.
The Four Classification Errors CMS Consistently Cites
Based on CMS’s ODAG audit protocol and the recurring patterns in program audit findings, four specific misclassification scenarios generate the most consistent conditions:
| Classification Error | What Actually Happened | CMS Audit Impact |
|---|---|---|
| Grievance logged as inquiry or general complaint | Member expressed dissatisfaction with a plan decision or service quality. Staff logged it as an informational call with no formal case opened. | Grievance timeliness clock never started. No written acknowledgment sent. Potential member rights violation. |
| Coverage request logged as grievance | Member or provider requested authorization for a service. Staff categorized the objection as a grievance rather than an organization determination request. | Organization determination timeline never triggered. Service access delayed without the required decision and notification process. |
| Standard appeal processed as expedited | Request received with no expedited language. Processor flagged expedited for speed. Universe submitted with incorrect case type. | IRE forwarding timeline discrepancy. Universe data integrity issue. Potential Star Rating data invalidity flag. |
| Expedited request processed as standard | Provider submitted expedited language. Intake staff or system did not recognize the expedited indicator and routed to standard queue. | Missed 24-hour deadline. Direct timeliness finding. Member potentially harmed by delayed authorization for time-sensitive care. |
Where Classification Actually Fails: The Intake Queue
Most compliance officers believe their classification problem is a training problem. In practice, it is more often a volume and channel-diversity problem that training alone cannot solve at scale.
A plan processing 500 A&G cases per month can address classification errors through intensive staff training and quality assurance review. A plan processing 5,000 cases per month across fax, mail, email, web, and phone — with documents arriving in inconsistent formats, with varying levels of completeness, from members, providers, AORs, and attorneys — has a structural problem that no amount of training resolves. The volume creates statistical inevitability of error. The channel diversity means no single staff member or team develops consistent expertise across every case type. The documentation inconsistency means the contextual cues that drive accurate classification are sometimes present and sometimes absent.
CMS’s audit protocol for ODAG grievances tests whether the plan correctly categorized each case in its universe. When CMS selects 15 grievance cases for review, a single misclassification in that sample generates a condition. Plans that process thousands of cases per month with manual intake workflows are running a statistical risk that grows proportionally with volume — not because of negligence, but because of the fundamental limitations of manual classification at scale.
The Timeliness Connection: Why Classification Is Also a Clock Problem
CMS’s timeliness standards for ODAG are unambiguous. Standard Part C organization determinations must be resolved within 14 calendar days for medical service requests. Expedited determinations must be resolved within 72 hours. Standard reconsiderations (appeals) must be resolved within 30 days for Part C. Expedited reconsiderations must be resolved within 72 hours.
Every one of these clocks starts at intake — at the moment the plan received the request, not the moment it was assigned to a reviewer or acknowledged in the case management system. When classification happens hours or days after receipt, the timeliness clock has already been running. And when classification is wrong, the clock may be running against the wrong standard, or not running at all.
This is why CMS’s industry-wide timeliness monitoring project collects data on all validated A&G universes annually — not just during formal program audits. The agency is running its own timeliness analysis, comparing plan-submitted data against the IRE’s forwarding data, and using discrepancies as evidence of universe data integrity issues that can trigger Star Rating data invalidity flags. Classification errors that produce incorrect case types in the universe don’t just affect the program audit score — they can affect Star Ratings independently.
Four Part C and D Star Rating appeal measures use data reported by sponsors to Maximus, the IRE. CMS cross-references this data against its own audit universe data and program audit findings. When the agency identifies data integrity issues — including classification-driven universe errors — it considers this as evidence that the contract’s measure data may be invalid and cannot be used in Star Ratings. A classification problem in your intake process can affect your Star Rating, not just your audit score.
What CMS Expects to See in a Compliant Intake Process
CMS does not prescribe the specific technology or workflow a plan must use for A&G intake. But the audit protocol and guidance make the expected outcomes clear. When auditors evaluate ODAG compliance, they look for:
- Consistent, documented classification of every received case against CMS-defined case type criteria — with evidence that the classification process is repeatable and not dependent on individual staff judgment
- Accurate expedited vs. standard determination at intake — with documentation that expedited indicators from providers were recognized and correctly applied
- Correct routing of each case type to the appropriate workflow with the appropriate timeliness clock initiated at receipt, not at assignment
- Evidence of quality monitoring over classification decisions, including regular review of intake accuracy and corrective action when patterns of misclassification are identified
- Universe data that accurately reflects the case type population — not what staff labeled cases, but what each case actually was under CMS’s definitions
The Action Plan for A&G Compliance Leaders
Audit your current classification error rate
Pull a sample of 50-100 cases from the last quarter and have your compliance team independently reclassify them using CMS’s criteria — without reference to how they were originally classified. The delta between your team’s classification and the original assignment is your structural error rate. Most plans that do this exercise are surprised by the magnitude.
Trace every timeliness miss back to classification
For every case in the last six months that missed its timeliness standard, examine whether the case was correctly classified at intake. How many timeliness deficiencies actually originated from a classification error that started the wrong clock? This analysis typically reveals that timeliness compliance is downstream of classification accuracy.
Map your intake channels to your classification consistency
Compare classification error rates by channel. Fax and mail typically produce higher error rates than portal submissions because the document structure is less predictable. If 80% of your classification errors originate from fax and mail intake, that is a channel-specific problem that requires a channel-specific solution.
Evaluate whether your case management system supports classification governance
Can you run a report showing all cases classified by a specific staff member over a given period? Can you identify cases where the initial classification was changed after assignment? Can you trace the original receipt timestamp against the classification timestamp to identify intake lag? If not, you cannot monitor your classification process systematically — and monitoring is what CMS expects.
See How Inovaare Automates A&G Classification at Intake
Inovaare’s AI Intake Agents automatically classify incoming appeals, grievances, and provider disputes against CMS criteria — with document extraction, expedited detection, and case generation built in. No manual classification. No intake lag. No universe data integrity risk.
Explore the Platform Request a DemoFrequently Asked Questions: Grievance Misclassification & ODAG Compliance
A grievance is a complaint about the quality, timeliness, or manner of care or service. An organization determination is a decision about whether a benefit is covered or a service is medically necessary. CMS requires Medicare Advantage plans to correctly distinguish between the two at intake, as they trigger different regulatory workflows and timeframes.
Grievance misclassification is one of CMS’s most recurring ODAG program audit findings. It appears across routine program audits and focus audits, and repeat findings can trigger Corrective Action Plans (CAPs) and civil monetary penalties.
Misclassification causes the case to bypass grievance-specific regulatory workflows — including acknowledgment letter timeframes, resolution deadlines, and member notification requirements. CMS reviewers will identify the original contact in call logs and cite the plan for processing failure, even if the underlying issue was eventually resolved.
Yes. AI-assisted classification tools can analyze incoming contacts in real time and apply decision-tree logic aligned with CMS definitions. When classification is ambiguous, the system can route cases to a supervisor for human-in-the-loop review — maintaining compliance while reducing manual classification error rates.
An ODAG (Organization Determinations, Appeals, and Grievances) universe is the structured dataset a health plan submits to CMS during a program audit. It includes all cases within the audit period across organization determinations, appeals, and grievances. Misclassified cases distort universe counts and trigger scope expansion during audit review.
Sources: CMS 2024 Part C and Part D Program Audit and Enforcement Report; CMS ODAG Audit Protocol; CMS Industry-Wide Part C Timeliness Monitoring Project; ATTAC Consulting Group ODAG Audit Analysis (2025)